Health
How HIV research has reshaped modern medicine
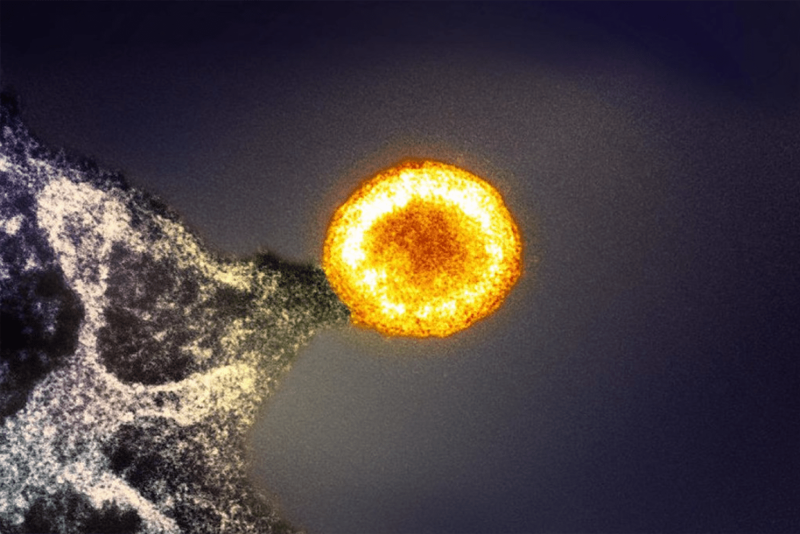
Colorized transmission electron micrograph of an HIV-1 virus particle (yellow/gold) budding from an infected cell.
Credit: NIAID/NIH
Decades of scientific work turned the tide on a fatal disease and yielded insights into immunity, vaccines, and more
In 1981, fresh out of medical school, physician-scientist Bruce Walker began his internship at Massachusetts General Hospital. One day, a young patient showed up with an unusual cluster of infections and cancers. Baffled and powerless to treat him, Walker and his colleagues could only watch as the patient quickly succumbed to the mysterious condition.
“I distinctly remember the first case we saw at Mass General,” said Walker, who is the Phillip T. and Susan M. Ragon Professor of Medicine at Harvard Medical School and the director of the Ragon Institute of Mass General, MIT, and Harvard. “The attending physician said that although we didn’t know what this condition was, we probably would never see another case like it.”
Two weeks later, another patient came in with the same set of symptoms. It quickly became clear to Walker and his colleagues that they weren’t dealing with a rare disease — it was the beginning of a new epidemic.
The baffling condition was acquired immunodeficiency syndrome (AIDS) — the most advanced stage of infection with the human immunodeficiency virus (HIV), which attacks and destroys infection-fighting immune cells. By 1993, HIV had become the leading cause of death in Americans aged 25-44 years.
In the 40-plus years since it was identified, scientists have made notable progress against HIV, transforming the infection from a death sentence into a manageable chronic condition, one that affects some 1.2 million people in the United States and nearly 40 million worldwide.
This decades-long quest for a cure for HIV has also yielded broader insights that have implications for the treatment of COVID-19, cancer, and other diseases.
From molecular insights to frontline medicines
Since the identification of HIV as the cause of AIDS, basic science and animal research have played a critical role in illuminating the virus’ complex behavior.
Some of the pivotal studies toward unraveling the structure, biology, and behavior of HIV have emanated from labs across Harvard Medical School. Using a range of imaging techniques, Stephen Harrison’s lab has identified key portions of HIV and studied the evolution of HIV antibodies, which is critical to understanding how the immune system interacts with the virus. The work of Joseph Sodroski, Bing Chen, and Alan Engelman has elucidated how HIV enters host cells and interacts with cell receptors, studying the structure and behavior of the virus’ protein envelope during this process.
This research has illuminated how HIV integrates its genetic material into host cell DNA, a crucial step in the virus’ life cycle. These insights have enhanced vaccine and therapeutic development by revealing how broadly neutralizing antibodies work and guiding the design of new immune-targeting strategies.
Early analyses of patient samples revealed that HIV is a human retrovirus — a type of virus that converts its RNA into DNA upon infecting a host cell. This tricks the host cell into copying the virus’ genetic material into its DNA as part of the cell’s normal replication cycle. The maneuver enables it to use the host cell machinery to make more viruses. HIV specifically goes after CD4 T lymphocytes or so-called helper T cells. These white blood cells coordinate immune response by signaling other immune cells to fight invaders. The virus begins by hijacking the cells’ molecular machinery to assemble thousands of viral particles, which go on to infect other CD4 T cells, spreading the pathogen throughout the body.
Today, the standard treatment for HIV is antiretroviral therapy (ART) — a combination of HIV medications, typically taken daily, that disrupt the virus’ replication cycle. When taken consistently, ART can lower the amount of actively replicating virus in the body — or viral load — to undetectable levels, lowering risk of transmission and allowing people with HIV to live nearly as long as uninfected individuals.
ART has also proved to be useful as a pre-exposure prophylaxis (PrEP) — an approach that can prevent up to 99 percent of sexually transmitted HIV infections from developing after exposure. Notably, a new class of medicines has raised hopes as a game-changer in HIV prevention. Two recent clinical trials of more than 7,500 cisgender men and transgender and nonbinary people showed that twice-a-year injections with the long-lasting drug lenacapavir prevented HIV infections in nearly all participants.
Yet, millions around the world are already infected. Once inside the body, HIV persists because of its remarkable ability to hide within healthy CD4 T cells, where it can lie dormant for years without triggering an immune response, said Daniel Kuritzkes, HMS Harriet Ryan Albee Professor of Medicine and chief of the division of infectious diseases at Brigham and Women’s Hospital.
Although these latent reservoirs of HIV do not actively produce new virus particles, they can reawaken at any time, leading to active HIV infection. This chronic immune activation among infected people — even when the virus is kept at bay — can amplify the risk for several chronic conditions.
“People living with HIV often have elevated markers of inflammation. This chronic immune activation can predispose people to long-term complications, including cardiovascular illness.”
Daniel Kuritzkes, chief of the division of infectious diseases, BWH
“People living with HIV often have elevated markers of inflammation,” Kuritzkes said. “This chronic immune activation can predispose people to long-term complications, including cardiovascular illness.”
Indeed, research has shown that people with HIV have a somewhat elevated risk for cardiovascular disease, diabetes, kidney disease, and certain types of cancer. Now, the latest research from Advancing Clinical Therapeutics Globally — a global network of experts conducting HIV research — has found that daily use of statins could reduce risk of cardiovascular disease in people living with HIV by 35 percent. This pivotal work was conceived by and led by Steven Grinspoon, HMS professor of medicine and director of the Metabolism Unit at Mass General Hospital.
While this offers a path toward managing HIV-related complications, Kuritzkes emphasizes that the ultimate quest of research efforts remains achieving sterilizing immunity through a vaccine that halts the virus in its tracks, preventing infection from taking hold in the first place.
The roadmap to a vaccine
With some 1.3 million new infections a year, a vaccine remains the best way to end the HIV epidemic, said Dan Barouch, the William Bosworth Castle Professor of Medicine at HMS and director of the Center for Virology and Vaccine Research at Beth Israel Deaconess Medical Center.
“We should use all of our prevention and treatment tools, including education and pre-exposure prophylaxis with antiretroviral drugs, to prevent HIV, but to really end the epidemic, we need a vaccine,” Barouch said.
Despite great strides with PrEP, Barouch notes, it will only reach high-risk individuals, and as many as half of new HIV infections occur in people who are not designated as high risk. Thus, Barouch notes, even if PrEP were available for free and accessible to everyone in the world, which is far from reality, it would still invariably reach a ceiling of population efficacy.
Yet, after 40 years of effort, the HIV vaccine field is at a crossroads. Since the dawn of HIV research, there have been hundreds of attempts at vaccine design, and dozens have made it to early-stage clinical trials, but only five have been tested in large-scale clinical trials.
“There is a lot of exciting basic, preclinical, and early clinical research, but currently no vaccine candidate has a clear trajectory for advanced clinical development,” Barouch said.
Why?
First, the ability of the virus to shapeshift within the host and across the population. The virus mutates rapidly, resulting in an astonishing genetic diversity not seen with any other virus.
“With HIV, you are not targeting a single virus, you’re targeting millions of different viruses,” said Barouch.
Another problem is the fact that the virus integrates itself into the host genome quickly — within days following infection — then goes into hiding, establishing a latent reservoir that can reactivate at any time. This means that a vaccine needs to induce rapid immune response that counters viral maneuvers very rapidly. No other virus seeds reservoirs so quickly, and no other vaccine has been capable of inducing such rapid defense.
Finally, the virus is cloaked in an envelope of sugar molecules — or glycans — that render it largely impervious to antibodies. There are only three or four targets on HIV that render it vulnerable to antibodies. Thus, for antibodies to work, they must be hyperprecise to latch on to these hotspots in order to disrupt the viral shield. This, Barouch notes, may be one of the greatest hurdles to developing a potent enough vaccine.
Among the most recent efforts was a vaccine developed by Barouch and Johnson & Johnson that was tested in Africa and in South and North America. The approach used a so-called “mosaic” platform optimized using computational biology to target multiple strains of the virus.
The researchers used computer design to create a mosaic antigen in the lab. The trial, which concluded in 2021, showed the vaccine had great safety but low efficacy — around 14 percent. A vaccine needs to be at least 50 percent effective, but ideally 70 percent or more, Barouch noted, meaning that it would have to prevent at least seven out of 10 infections.
Despite the disappointing results, Barouch said, the findings helped refocus the field of HIV vaccine research on the importance of neutralizing antibodies — the types of immune proteins that are capable of disabling rather than merely recognizing the virus.
To that end, Barouch and team have redoubled their efforts to design vaccines that create precisely such broadly neutralizing antibody response as well as spark a robust T cell response, thus activating both major arms of the immune system.
Lessons from elite controllers
In the early 1990s, researchers noticed a tiny subset of HIV-infected patients who were living healthy and symptom free without medication. These patients, who came to be known as elite controllers, had undetectable viral levels in their bodies. Their immune systems were powerful enough to naturally keep the virus from replicating. Between 0.15 and 1.5 percent of HIV-infected individuals are estimated to be elite controllers.
“In these individuals, the immune system is able to suppress HIV replication,” said Yu, whose lab focuses on the molecular and cellular mechanisms behind this remarkable immune response, with the hope of harnessing these insights to develop new antiretroviral treatments for HIV. “And in a rare subgroup, the immune system may even eliminate all cells infected with replication-competent HIV, curing the infection entirely.”
When Gaurav Gaiha, then a first-year student in the Harvard-MIT Program in Health Sciences and Technology, learned about elite controllers, he was captivated by the concept of using insights from these unique individuals to develop an HIV vaccine.
At that time, a prevailing scientific theory was that elite controllers had an exceptionally powerful T cell response to HIV. However, when Gaiha began comparing the T cell responses in elite controllers to that of people living with progressive HIV, he discovered something surprising: While T cell function in elite controllers was important, there was another important piece to this biological riddle. Gaiha therefore shifted his focus and instead began to zero in on the specific regions of the virus that these T cells were targeting.
In a 2019 study, Gaiha, Walker, and colleagues applied network theory to tackle this question. They treated each amino acid in the viral proteins as a node in a network, allowing them to quantify how central each amino acid was to the protein’s function. Their findings offered a breakthrough: T cells in elite controllers consistently targeted critical regions of the virus protein network — areas that were essential for its survival and losing or mutating them would significantly hinder the virus’ ability to replicate.
“It’s similar to key players in a network,” said Gaiha, now an assistant professor of medicine at HMS and a principal investigator at the Ragon Institute of Mass General, MIT, and Harvard. “Key players keep the network connected, while others may be more on the periphery. If T cells target key player amino acids from these critical regions of viral proteins, you may have a chance to control the virus for a long period of time without therapy.”
These insights, Gaiha noted, have implications beyond HIV — they helped guide COVID-19 vaccine developments that stimulate T cells and induce a robust and long-lasting immune response.
Encouraged by promising results in humanized mice, Gaiha and Walker are now collaborating with two biotech companies to translate these insights into a viable HIV vaccine. The group’s viral vector-based vaccine candidate is set to enter a first in human clinical trial in Zimbabwe and South Africa in early 2025, while a second RNA-based vaccine trial is meant to begin in 2026 at Mass General.
“I am hopeful that we will see good outcomes from these initial vaccine trials,” said Gaiha. “But more importantly, I am looking forward to learning key lessons that will guide us, so we can continue to refine. We’re in this for the long haul.”
Ripple benefits beyond HIV
The search for a cure continues, but the sinuous 40-plus-year journey has fueled advances well beyond HIV.
For starters, many of the successes in the identification, testing, and treatment of SARS-CoV-2, the virus that ignited the COVID-19 pandemic, were built on knowledge and hard-earned experiences with HIV.
“Research on HIV really paved the way for the advances that were made with COVID, by laying the platforms for vaccine development that, in particular, the vectors that were used to generate immune responses, the mechanisms for rapid diagnostics, the understanding of viral pathogenesis — all were really contributed by work that had been done on HIV,” Walker said.
“If it wasn’t for the decades of HIV research, we would not have had the COVID-19 vaccines so rapidly.”
Dan Barouch, director of the Center for Virology and Vaccine Research, BIDMC
“If it wasn’t for the decades of HIV research, we would not have had the COVID-19 vaccines so rapidly,” Barouch said.
HIV research also equipped scientists with the tools and know-how to unravel viral structures and monitor the behavior of viruses inside their hosts. This work also led to the development of animal models that allow researchers to study how the body responds to vaccines and treatments and laid the foundation for the modern-day infrastructure needed to conduct clinical trials.
HIV research has catalyzed understanding of immune system function in myriad ways. For example, recent advances in gene therapy and CAR T cells were heavily influenced by research conducted in HIV infection.
“Fundamental mechanisms of how the immune system can recognize, engage, and target virally infected cells were first discovered in the context of HIV infection, and a lot of this progress has subsequently been translated to alternative disease contexts,” said HIV researcher Xu Yu, professor of medicine at HMS and a principal investigator at the Ragon Institute of Mass General, MIT, and Harvard.
For example, gene therapy uses lentiviruses as vectors to deliver therapeutic genes into the target cells.
“These lentiviruses are very similar to HIV, and a deeper understanding of HIV allowed researchers to use lentiviruses for therapeutic gene transfer,” Yu said.
HIV research also helped advanced the field of CAR T-cell therapy, which uses genetically engineered immune cells for the treatment of blood cancers. One of the first CAR T-cell studies was done in the context of treating HIV infection, more than 20 years ago.
“Experience gained with CAR T cells in this setting was instrumental in advancing them for oncologic indications,” Yu said.